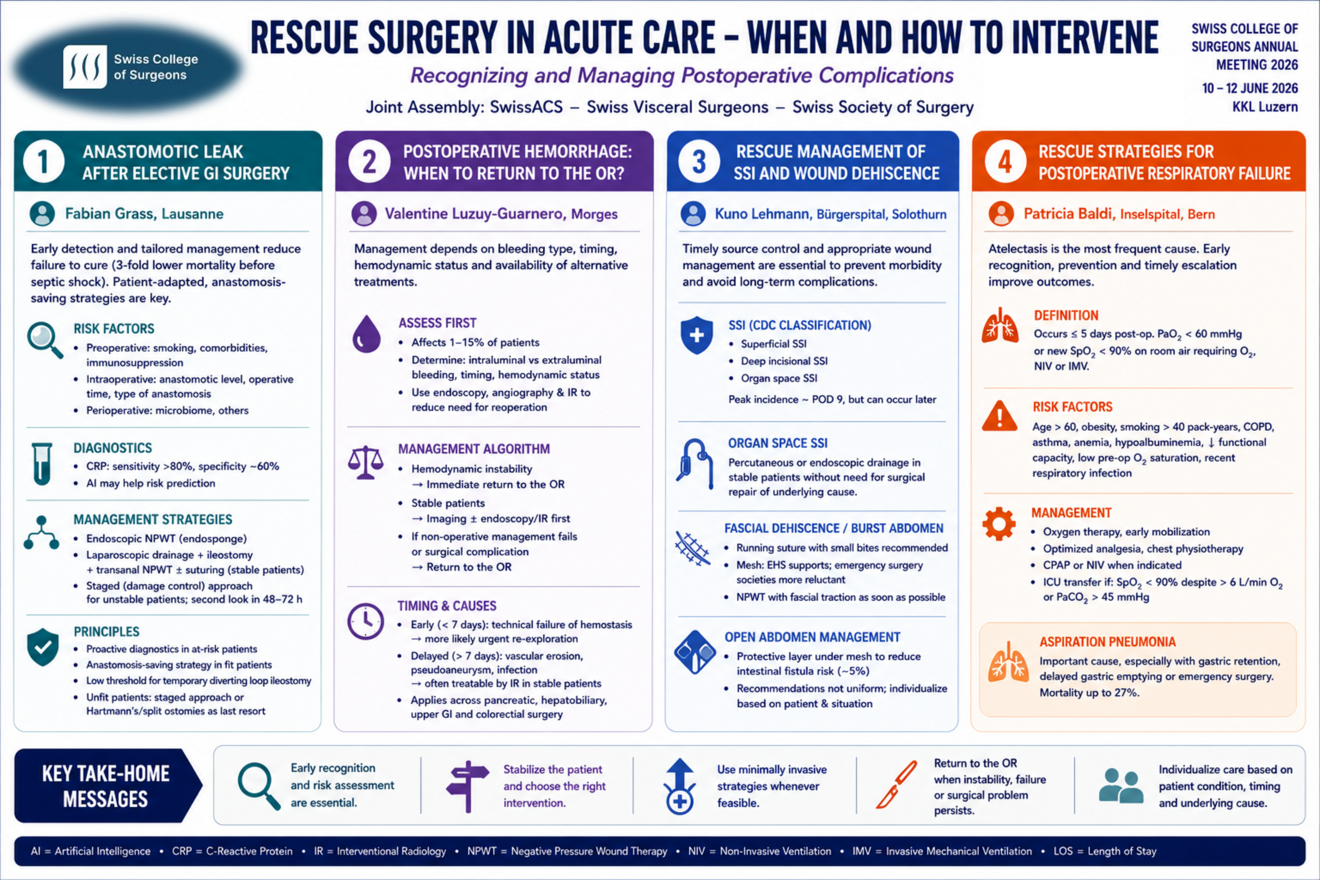





Session summary of a joint assembly of the Swiss Society of Trauma & Acute Care Surgery (SwissACS), Swiss Visceral Surgeons and the Swiss Society of Surgery at the SWISS COLLEGE OF SURGEONS ANNUAL MEETING 2026, 10 – 12 JUNE 2026, KKL Luzern
Session Introduction
Beat Schnüriger, Bern
This introductory presentation focuses on the importance of rescue strategies for major postoperative complications following elective gastrointestinal (GI) surgery. While surgical complications cannot always be prevented, patient outcomes depend heavily on the ability to recognize complications early and intervene promptly and effectively.
A central concept is "failure-to-rescue," which refers to the inability to prevent death after a major complication has occurred. This metric is increasingly regarded as an important indicator of healthcare quality. The presentation emphasizes that early diagnosis, structured monitoring, and timely intervention can significantly alter a patient's clinical course.
Key learning objectives include:
– Recognizing the early warning signs of major postoperative complications.
– Understanding current rescue strategies for:
Anastomotic leaks
Postoperative hemorrhage
Surgical site infections and wound dehiscence
Postoperative respiratory failure
– Identifying factors that improve successful rescue and reduce failure-to-rescue rates.
– Applying practical management principles in everyday clinical practice.
Overall, the presentation introduces a proactive approach to postoperative care, emphasizing that effective rescue strategies are just as important as preventing complications and play a crucial role in improving surgical outcomes.
Recognizing and managing anastomotic leak after elective GI surgery
Fabian Grass, Lausanne
Anastomotic leaks (AL) represent inevitable and most feared complications after colorectal resections. Risk factors for AL are multifold and widely described in the literature, and may be related to preoperative (i.e. smoking, comorbidities, immunosuppression), intraoperative (anastomotic level, operative time, type of anastomosis) and perioperative (i.e microbiome) risk factors. A high degree of suspicion in patients at risk, timely recognition to prevent failure to cure, and a tailored management plan adapted to the patient’s condition are of utmost importance, together with careful intra- and postoperative decision making. According to a recent study (Savitch JAMA Surg 2026), early leak detection before septic shock occurs is associated with a 3-fold decreased failure to cure (mortality within 30 postoperative days) rate. While artificial intelligence methodology may help with risk prediction, C-Reactive Protein remains a widely used marker of AL in the early postoperative period, however with a low specificity (60%) despite a high sensitivity of >80%. In terms of management strategies, endoscopic techniques such as negative pressure wound therapy (NPWT) devices (endosponge) gained popularity, together with a trend to more anastomosis saving approaches in selected patients, mainly to avoid long-term ostomies especially in the younger and fit population. While endosponge treatment requires a long hospital stay and often multiple interventions, the mortality rate is low. In stable patients, a laparoscopic approach with drainage and ileostomy creation combined with transanal NWPT and suturing of the defect may thus represent the preferred option. On the other hand, a staged procedure (damage control surgery) to stabilize an unstable patient with a planned second look to safe or redo the anastomosis 48-72 hours later may represent an option in selected patients to avoid long term ostomies.
Taken together, proactive diagnostics in patients at risk and elaboration of an anastomosis saving strategy especially in low AL gain interest. In fit patients, owersewing or redoing a more proximal primary anastomosis deserves consideration, with a low threshold for a temporary diverting loop ileostomy. In unfit patients, a staged (damage control) approach or, as a last resort, Hartmann’s or split ostomies remain the safest choice.
Postoperative Hemorrhage: When to Return to the OR?
Valentine Luzuy-Guarnero, Morges
Postoperative hemorrhage is one of the most feared complications after abdominal surgery, affecting 1–15% of patients depending on the procedure and carrying significant morbidity and mortality. The main challenge is determining when surgical re-exploration is required. Management depends on the type of bleeding (intraluminal or extraluminal), its timing, the patient’s hemodynamic status, and the availability of alternative treatments such as endoscopy, angiography, or interventional radiology.
A key principle is that hemodynamic instability generally mandates immediate surgical intervention, whereas stable patients should first undergo diagnostic imaging and, when appropriate, less invasive therapeutic procedures. Advances in endoscopy and interventional radiology have substantially reduced the need for reoperation and have become central to the management of postoperative bleeding across abdominal surgical specialties.
Although the underlying causes vary by procedure, early hemorrhage is most often related to technical failure of hemostasis and is more likely to require urgent re-exploration. In contrast, delayed bleeding is frequently associated with vascular erosion, pseudoaneurysm formation, or infectious complications and can often be managed successfully with interventional radiology in stable patients. This approach is now widely applied in pancreatic, hepatobiliary, upper gastrointestinal, and colorectal surgery.
Overall, postoperative hemorrhage management follows a stepwise strategy that prioritizes minimally invasive techniques whenever feasible. Nevertheless, relaparotomy remains the treatment of choice in patients with hemodynamic instability, failed non-operative management, or surgical complications requiring definitive correction.
Rescue management of surgical site infections (SSI) and wound dehiscence
Kuno Lehmann, Bürgerspital, Solothurn
Surgical site infections are a common cause of postoperative morbidity. The CDC defines three categories: Superficial SSI, deep incisional SSI and organ space SSI. Peak incidence is around postoperative day nine, but all of them can occur at later timepoints. A major issue of deep incisional and organ space SSI is the frequent need for surgical reintervention. Percutaneous or endoscopic management of organ space SSI is possible in stable patients without a need for surgical repair of an underlining cause. In patients with burst abdomen (fascial dehiscence), the need for reintervention is obvious. Currently, a running suture with small bites is recommended for closure – like any primary closure of a laparotomy. Interrupted sutures are propagated by some groups – a high-quality head-to-head comparison is not available. The use of a synthetic mesh is recommended by the EHS (European Hernia Society); however, emergency surgery societies (e.g. WSES) are more reluctant. Recommendations for the management of open abdomen – mostly used to treat or prevent abdominal hypertension (compartment syndrome) are not uniform. Again, the EHS supports the use of a synthetic mesh for definitive closure, while emergency surgery societies remain sceptic. Everyone agrees on the use of NPWT (negative pressure wound therapy) with facial traction as soon as possible to avoid retraction of the ventral muscles. A protective layer should be used below the mesh to reduce the risk of intestinal fistula – which remains at 5%.
Rescue Strategies for Postoperative Respiratory Failure
Patricia Baldi, Inselspital, Bern University Hospital, Bern
Postoperative respiratory failure is a serious complication occurring within five days after surgery and is defined by a PaO₂ < 60 mmHg or a new-onset SpO₂ < 90% on room air requiring oxygen therapy, non-invasive ventilation, or invasive mechanical ventilation. It is associated with increased morbidity, mortality, ICU admissions, prolonged hospital stay, and higher healthcare costs. Common postoperative pulmonary complications are atelectasis, pneumonia, pulmonary edema, hypoxemia after extubation, and reintubation. Risk factors are age > 60 years, obesity, smoking > 40 pack-years, COPD, asthma, anemia, hypoalbuminemia, reduced functional capacity, low preoperative oxygen saturation, and recent respiratory infections. Atelectasis is the most frequent cause and results from high inspired oxygen concentrations, anesthesia-induced diaphragm dysfunction, postoperative pain, and reduced lung expansion. Management includes oxygen therapy, early mobilization, optimized analgesia, chest physiotherapy, CPAP or NIV when indicated, and ICU transfer in cases of progressive respiratory failure (SpO₂ < 90% despite > 6 L/min oxygen or PaCO₂ > 45 mmHg). Aspiration pneumonia is another important cause of postoperative respiratory failure, particularly in patients with gastric retention, delayed gastric emptying, or emergency surgery, and is associated with a mortality rate of up to 27%.
Key References: Ranieri et al., 2012; Canet & Gallart, 2014; Canet et al., 2015; Miskovic & Lumb, 2017; Eikermann et al., 2019; Munshi et al., 2022; Lagina & Valley, 2024; Palermo et al., 2024; Ranjha & Gilbert, 2026; Nava & Hill, 2009; Studer et al., 2016.