
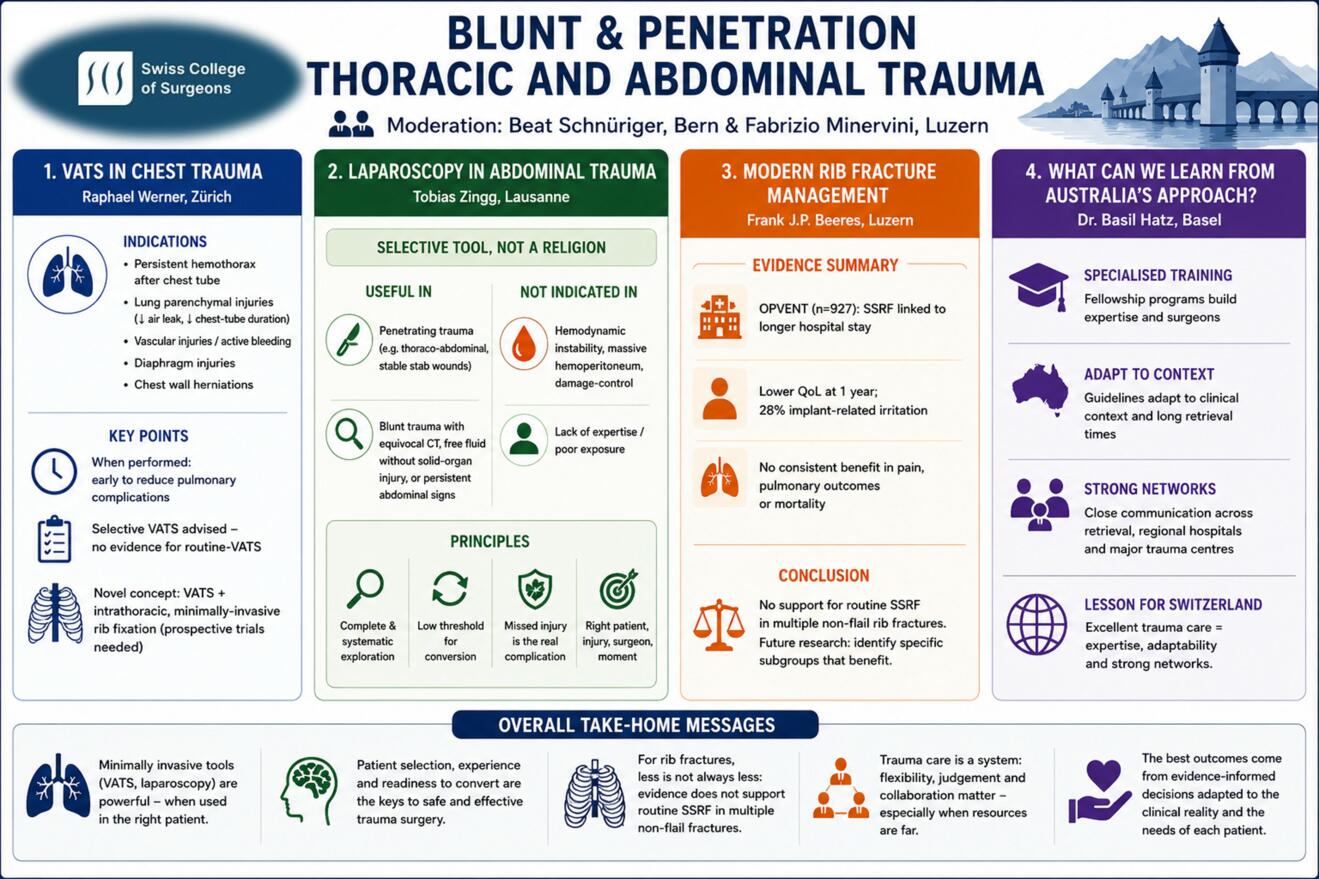



VATS in Chest Trauma – Indications & Applications
Raphael Werner, Zürich
VATS has become a useful tool in the management of chest trauma and is indicated primarily for the treatment of associated intrathoracic injuries: the evacuation of persistent hemothorax after chest tube placement, the treatment of lung parenchymal injuries (thereby reducing air leak and chest-tube duration), repair of vascular injuries and assessment of active bleeding in patients with hemothorax, the treatment of diaphragm injuries and closure of chest wall herniations.
Current guidelines (ACS/CWIS; WSES/AAST) note that VATS at the time of surgical stabilization of rib fractures may offer a pulmonary improvement by evacuation of retained hemothorax or recurrent effusion, but there are no definitive data favoring routine-VATS over selective-VATS on a case-by-case decision. When VATS is performed, it should be done early to reduce pulmonary complications and prevent secondary interventions.
Recently, a novel strategy combines VATS with intrathoracic, minimally-invasive, muscle-sparing rib fixation. However, prospective trials are needed to investigate the clinical benefit of intrathoracic rib fixation over conventional rib stabilization.
Laparoscopy in abdominal trauma: a selective tool, not a religion
Tobias Zingg, Lausanne
Laparoscopy has gained an established but selective role in the management of abdominal trauma. It should not be considered a substitute for trauma laparotomy or damage-control surgery, but rather as a tool to improve patient selection, avoid unnecessary laparotomies, diagnose occult injuries, and treat selected lesions in stable or compensated patients.
The first indication for laparoscopy is not a specific CT finding, but physiological stability. Patients with persistent hypotension, ongoing transfusion requirements, massive hemoperitoneum, abdominal compartment physiology, poor exposure, or lack of adequate expertise should proceed to laparotomy or damage-control management. In contrast, laparoscopy may be useful in stable patients without an immediate indication for open surgery, provided that an experienced laparoscopic surgeon and an operating room team prepared for immediate conversion are available.
In penetrating trauma, laparoscopy has one of its clearest indications. It is particularly valuable in thoraco-abdominal injuries, where small diaphragmatic lesions may be missed on CT and can later result in delayed herniation. In stable anterior abdominal stab wounds, laparoscopy may also be used as part of a selective strategy to assess peritoneal violation, exclude diaphragmatic injury, and detect occult bowel or mesenteric lesions. Its main benefit in this setting is the reduction of non-therapeutic laparotomies, but this benefit must never come at the cost of a missed hollow viscus injury.
In blunt abdominal trauma, the role of laparoscopy is more limited and more controversial. It is not indicated for unstable solid-organ bleeding or damage-control situations. Its main value lies in suspected bowel or mesenteric injury, particularly when CT findings are equivocal, when free fluid is present without solid-organ injury, or when abdominal signs persist despite initial non-operative management. In this context, laparoscopy can help clarify diagnosis and, in selected cases, allow therapeutic repair.
The safety of trauma laparoscopy depends on complete and systematic exploration: both diaphragms, the small bowel from Treitz to the ileocecal valve, the colon, and the mesentery must be inspected. Conversion should not be regarded as failure, but as part of the strategy. In trauma laparoscopy, the complication is not conversion; the complication is missed injury.
The future of laparoscopy in abdominal trauma is therefore not maximal minimal invasiveness, but better selection: the right patient, the right injury, the right surgeon, and the right moment.
Modern Rib Fracture Management
Frank J.P. Beeres, Luzern
Surgical stabilization of rib fractures (SSRF) has gained increasing acceptance; however, its role in patients with multiple non-flail rib fractures remains controversial. This presentation critically reviews the current evidence, focusing on patients with ≥3 rib fractures who are neither ventilated nor have a flail chest. Key studies, including OPVENT, NON-FLAIL, and RIB-FIX, demonstrate considerable methodological challenges, such as selection bias, limited randomization, and strong treatment preferences among patients and surgeons.
Data from the prospective multicenter OPVENT study (n = 927) showed that SSRF was associated with a longer hospital length of stay compared with non-operative management. At one-year follow-up, surgically treated patients reported lower quality-of-life scores, while 28% experienced implant-related irritation. No consistent improvements were observed in pain, pulmonary outcomes, or mortality.
Contemporary non-operative management, consisting of multidisciplinary care, optimized analgesia, and physiotherapy, achieves favorable outcomes, including low mortality, acceptable complication rates, and quality-of-life measures comparable to the general population.
Current evidence does not support routine SSRF in patients with multiple non-flail rib fractures. Future research should focus on identifying specific patient subgroups that may benefit from surgical intervention rather than expanding operative indications broadly.
What can we learn from Australia’s approach?
Basil Hatz, Basel
While modern trauma care is built on evidence-based protocols and rapid access to specialist services, Australia frequently requires clinicians to manage severely injured patients hundreds of kilometres away from a major trauma centre. This reality demands flexibility, clinical judgement, and strong collaboration across the entire trauma network.
Drawing on experiences from a trauma fellowship in Perth, Western Australia: First, dedicated trauma fellowship programs provide invaluable exposure to high-acuity trauma and foster the development of highly specialised trauma surgeons. Second, guidelines should not be applied rigidly but adapted to the clinical context. In environments where retrieval times may exceed the golden hour, treatment decisions must consider not only the patient’s current condition but also how that condition may evolve during prolonged transport. Finally, close communication between retrieval services, regional hospitals, and major trauma centres is essential to ensure safe and effective patient care.
The Australian experience demonstrates that excellent trauma care relies not only on protocols but also on expertise, adaptability, and strong networks. These lessons are equally relevant for the trauma system in Switzerland.









