Case Description:
A 78-year-old male patient presented to the emergency department with absent bowel movements for 4 days and increasing abdominal pain and cramps. He is currently undergoing oncological treatment with radio-chemotherapy for a squamous cell carcinoma of the oropharynx. Parkinson's disease, hypertension, and sick sinus syndrome with atrial fibrillation are treated with medication.
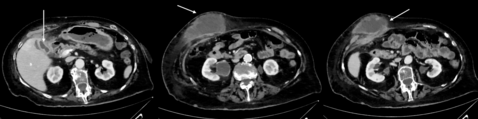
Physical examination reveals a distended abdomen with tenderness in all quadrants, but no evidence of peritonitis. A percutaneous endoscopic gastrostomy (PEG) tube in the upper abdomen was inserted a few days ago without complications and can be flushed without problems. Blood results showed a normal leukocyte count of 3.77 and an elevated CRP of 142 mg/l without any other abnormalities. An abdominal x-ray and CT scan (Figure 1.) was performed and showed a sigmoid volvulus without free air or signs of ischemia. The patient was referred to gastroenterology for endoscopic detorsion. The patient was discharged four days later, after an uneventful course.
Five days later, the patient represented to the emergency department because he again experienced lower abdominal pain and cramps without bowel movements since hospital discharge. Another sigmoid volvulus was diagnosed radiologically and the patient underwent another successful endoscopic detorsion. A mechanical bowel prep was given but the next day, stool passage was still not observed and the patient presented with an increasingly distended abdomen. To our surprise, abdominal radiography showed the third time a sigmoid volvulus. As before, endoscopic detorsion was successfully performed, and this time additionally “stented” with a large
rectal tube as prophylaxis of another volvulus.

Figure 1
What should be the next step in the management of this patient?
A Stepwise withdrawal of colonic tube and discharge with laxatives
B Emergency laparoscopic sigmoidopexy
C Laparoscopic sigmoidectomy the next day
D Percutaneous endoscopic sigmoidopexy
Case Solution:
C
Volvulus is a torsion of any segment of the alimentary tract, whereby the sigmoid colon and cecum are the most common sites(1). The exact pathophysiology is not fully clear, but there are risk factors reported in the literature: Anatomic reasons such as an enlarged, flexible sigmoid with a narrow mesentery and colonic dysmotility (e.g. longer transit time) or infection (Shagas disease)(2). Elderly men are more frequently affected by sigmoid volvulus(2). Recurrence after endoscopic detorsion alone is reported to be as high as 85%(3). Diagnosis is usually made by abdominal radiography or CT scan showing proximal dilatation of the colon or whirl pattern(4).
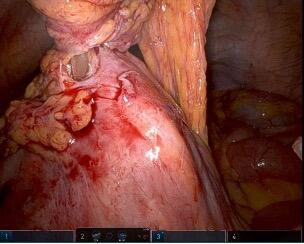
Therapy is dependent on the patient’s status and radiological findings. The diagnosis of a ceacal volvulus is an indication for surgery(5). A patient with a sigmoid volvulus with signs of peritonitis or perforation should undergo emergency resection of the volvulized colon(6). Otherwise, endoscopic detorsion of the sigmoid followed by resection is recommended, as non-resectional surgery, such as pexy, showed inferior results(7, 8). In our case, sigmoid resection during the first hospital stay was not performed due to ongoing chemotherapy. However, elective sigmoid resection was scheduled with the diagnosis of recurrent sigmoid volvulus. During surgery, the unexpected reason for the recurrent (or persistent) sigmoid volvulus was detected (Figure 2.):
The PEG tube pierced the sigmoid colon fixing it in a rotated way to the feeding tube in the upper abdominal quadrant causing bowel obstruction and the radiological image of a volvulus. The postoperative course was uneventful and patient was discharged a few days later.
- Ballantyne GH, Brandner MD, Beart Jr R, Ilstrup DM. Volvulus of the colon. Incidence and mortality. Annals of surgery. 1985;202(1):83.
- Bauman ZM, Evans CH. Volvulus. Surgical Clinics. 2018;98(5):973-93.
- Chung Y, Eu K, Nyam D, Leong A, Ho Y, Seow-Choen F. Minimizing recurrence after sigmoid volvulus. Journal of British Surgery. 1999;86(2):231-3.
- Catalano O. Computed tomographic appearance of sigmoid volvulus. Abdominal imaging. 1996;21:314-7.
- Alavi K, Poylin V, Davids JS, Patel SV, Felder S, Valente MA, et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Colonic Volvulus and Acute Colonic Pseudo-Obstruction. Dis Colon Rectum. 2021;64(9):1046-57.
- Vogel JD, Feingold DL, Stewart DB, Turner JS, Boutros M, Chun J, et al. Clinical practice guidelines for colon volvulus and acute colonic pseudo-obstruction. Diseases of the Colon & Rectum. 2016;59(7):589-600.
- Naveed M, Jamil LH, Fujii-Lau LL, Al-Haddad M, Buxbaum JL, Fishman DS, et al. American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in the management of acute colonic pseudo-obstruction and colonic volvulus. Gastrointestinal endoscopy. 2020;91(2):228-35.
- Larkin J, Thekiso T, Waldron R, Barry K, Eustace P. Recurrent sigmoid volvulus–early resection may obviate later emergency surgery and reduce morbidity and mortality. The Annals of the Royal College of Surgeons of England. 2009;91(3):205-9.