


This study, “Determining safe washout period for immune checkpoint inhibitors prior to liver transplantation,” is a collaborative, multicenter cohort investigation led by the transplant group at the University Hospital of Geneva. It evaluates the safe use of immune checkpoint inhibitors (ICIs) before liver transplantation (LT) in patients with liver cancer and more specifically hepatocellular carcinoma (HCC). The introduction of ICIs for HCC has expanded eligibility for LT for patients with a favorable response to ICI, enabling patients previously unsuitable for surgical intervention to become candidates for potentially curative LT. However, the immunostimulatory effects of ICIs increase the risk of graft rejection. This study aimed to determine the optimal interval between ICI discontinuation and LT to minimize rejection risk without increasing the recurrence risk.
We performed a structured search to identify studies reporting on patients with HCC who received ICI therapy before LT. Study authors and additional LT expert centers were contacted to provide additional patient data. Survival analysis focused on two primary adverse events: allograft rejection (including graft loss) and HCC recurrence. We analyzed relevant variables included HCC-related factors (staging, tumor burden), ICI-related factors (regimen, duration, washout period), and transplantation-related factors (ischemic times, graft types).
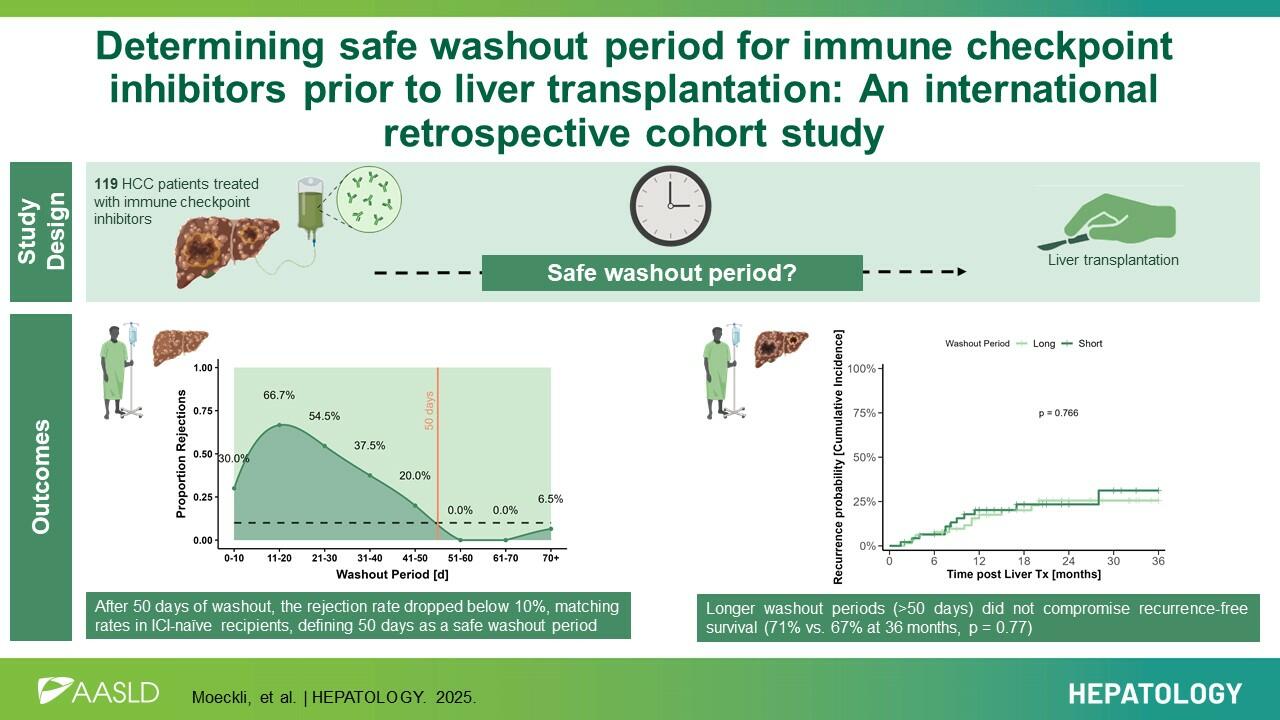
Allograft rejection occurred in 20.2% of patients (24/119). Logistic regression analysis identified shorter washout periods as a significant risk factor for rejection. A washout period of 50 days or more was associated with a substantially lower rejection risk. HCC recurrence occurred in one fifth of patients, but no association was found between washout duration and recurrence risk.
This study establishes a 50-day washout period as safe for patients undergoing ICI therapy before liver transplantation, offering a clear path to expand transplant eligibility for HCC patients without compromising safety. By defining this threshold, our findings enable broader use of ICIs as effective downstaging and bridging tools, providing access to curative transplantation for patients who achieve sufficient disease control. Our findings have the potential to find their way into clinical guidelines in the near future. Eventually we anticipate that more HCC patients will benefit from life-saving transplants in the coming years without risking high rejection rates. As ICI therapies continue to gain territory, our results lay the foundation for integrating them safely and effectively into transplantation pathways worldwide.
Interview with Dr. med. Beat Möckli (Genève)
What inspired you to conduct this study?
We were frequently confronted with patient presentations during multidisciplinary tumor board where ICI therapy was held or delayed due to a high position on the liver transplantation waiting list. While everyone was scared of the risk of the risk of rejection, it was frustrating to face a lack of data on the safe washout period and to rely on data from anecdotal case reports. We wantedto address this lack of data.
Additionally, our lab is currently working on a basic science research project exploring the use ofICI in the context of liver surgery and transplantation, which further motivated us to address thisgap in clinical knowledge and connect clinical and basic science research.
Were there any unexpected findings?
Although we hypothesized that longer washout periods would correlate with higher HCCrecurrence rates, statistical analyses did not support this association. Those findings suggest that transplantation remains safe in terms of recurrence risk for the washout periods studied which was 50 day.
Additionally we expected that a lower graft quality would increase the risk of rejection and therefore placed particular emphasis in our study on graft related factors. This proved to be wrong and our data did not show an influence of graft related factors on the rejection risk.
What is the direct impact on the surgeon's work?
These results will help establish clear guidelines on the washout period for ICI therapy before LT, providing surgeons with a concrete framework for decision-making on when to stop ICI. Also, patients previously considered candidates for palliative care may now have a higher chance of being placed on ICI by their oncologists, potentially making them eligible for curative transplantation. More directly related to our daily work as surgeons, this study underscores that surgical decision-making does not occur in isolation. We must consider all patient-related factors, particularly new biologic and targeted therapies, to provide optimal treatment with the best possible timing.
What is your learning point from this project?
This project demonstrated both the power and challenges of conducting collaborative multicentric studies. By pooling data from 29 centers across Europe, Asia, and North America, we were able to gather a diverse dataset that provided the statistical power necessary to address a clinically relevant question that no single center could have resolved independently.
However, coordinating data collection across multiple sites posed significant logistical challenges, including differences in data quality, variable adherence to protocols, and the need for multiple reminder emails to certain study sites.
Are there any subsequent projects planned?
One unexpected observation of our study was that multiple patients developed graft-versus-host disease (GVHD), an occurrence that is exceedingly rare in liver transplantation. This raises the question of whether GVHD could represent another manifestation of immunological adverse events following ICI therapy. Investigating this possibility would be an intriguing question for a next study.






