A suspected abscess in the right upper abdominal quadrant was the reason for referral of a 95-year old patient to our emergency department. Laboratory results and computed tomography images confirmed the suspected diagnosis. Due to her comorbidities a best supportive care approach was established.
Case Description
A 95-year-old patient was assigned to our emergency department by her family doctor due to a suspected abscess in the right upper abdominal quadrant. Redness and swelling were noticed by the caregivers of the patient three days prior to admission.
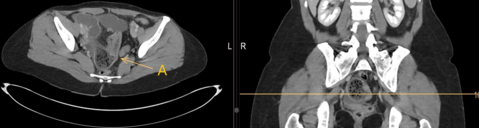
The patient suffered from dementia and therefore further anamnesis with the patient was not possible. The caregivers of the patient did not notice any change in the general condition of the patient. Physical examination revealed a right upper quadrant mass, approximately the size of a tennis ball, with pain on palpation (Figure A).

Figure A: palpable mass in the right upper quadrant
The patient was subfebrile with a temperature of 37.1°C with normal blood pressure (126/76 mmHg) and tachycardia (122 bpm). The laboratory tests indicated an inflammation with a leukocytosis of 16.8x109/l and a CRP of 157 mg/l. The family doctor started an oral therapy with co-amoxicillin one day before admission, which had not yet shown any reduction of the symptoms. The patient’s other diagnoses apart from dementia were arterial hypertension, coronary heart disease and diabetes. Due to the suspected intraabdominal origin of the inflammation, we performed a CT scan which showed the following results (Figure B).
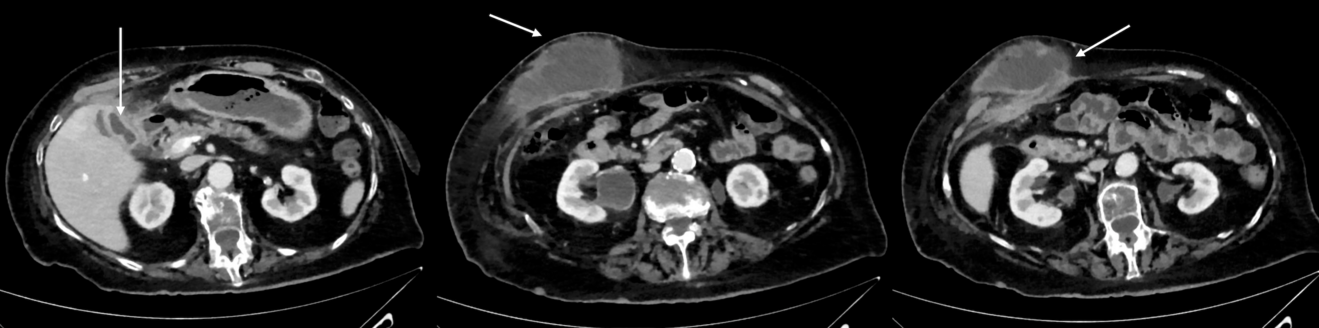
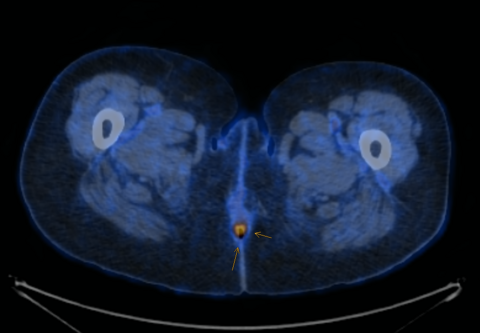
Figure B: arrows from left to right: subcutaneous mass, perforation of abdominal wall, gallblader
What is the most probable diagnosis?
A) Subcutaneous abscess
B) Infected atheroma
C) Pyogenic liver abscess
D) Cholecystocutaneous fistula
E) Perforated right side colonic malignancy
Case Solution
The CT scan revealed a cholecystocutaneous fistula, which is a rare complication of neglected cholecystitis with or without calculi or gallbladder carcinoma (1–3). A persistent or recurrent subcutaneous abscess with purulent or bile-stained discharge and systemic inflammatory signs such as fever is the most common presentation (4). In fact, our patient showed the typical symptoms and the family doctor suspected an abscess accordingly. Accompanying findings were a pleural effusion and a lower lobe atelectasis.
Nowadays, cholecystocutaneous fistulas are extremely rare, but they were first described as early as 1670 (2,5). The typical patients are, as in our case, elderly women (2). As the incidence of cholecystocutaneous fistulas is very low, there are no treatment standards (2). However, if the patient is eligible for a surgical treatment, open or laparoscopic cholecystectomy and excision of the fistula is the therapy of choice (2,5). Less invasive options are interventional abscess drainage and singular antibiotic treatment (2,3).
Our patient was offered a surgical approach with cholecystectomy and excision of the fistula. As the patient suffered from dementia and could no longer make any medical decision, we discussed all the possible treatment strategies with her family. The patient was 95 years old and suffered from highly advanced dementia, consequently her family decided on a palliative approach with neither surgery nor antibiotic treatment. Therefore, we discharged the patient back to the nursing home where she received comfort care. As a result of the untreated inflammation, the abscess eventually perforated the abdominal wall and the patient passed away a few days after.
1. Kapoor Y, Singh G, Khokhar M. Spontaneous cholecystocutaneous fistula-not an old time story. Indian J Surg. 2013 Jun;75(Suppl 1):188–91.
2. Brimo Alsaman MZ, Mazketly M, Ziadeh M, Aleter O, Ghazal A. Cholecystocutaneous fistula incidence, Etiology, Clinical Manifestations, Diagnosis and treatment. A literature review. Ann Med Surg (Lond). 2020 Nov;59:180–5.
3. Gupta V, Benerjee S, Garg H, Vyas S. Spontaneous cholecysto-antral-cutaneous fistula: a consequence of neglected calculus cholecystitis. Singapore Med J. 2012 Oct;53(10):e201-3.
4. Ayoub K, Alkarrash M shadi, Shashaa MN, Zazo A, Rhayim R, Mahli N. A rare complication of gallstones ended with spontaneous cholecystocutaneus fistula in an old man: A case report. Int J Surg Case Rep. 2020 Jan 1;67:42–4.
5. H S Flora and S Bhattacharya. Spontaneous cholecystocutaneous fistula. HPB (Oxford). 2001;