


Introduction
The term pancreatic cystic neoplasms (PCN) summarizes a heterogenous group of pancreatic cysts such as intraductal papillary mucinous cystic neoplasms (IPMN), mucinous cystic neoplasm (MCN) and serous cystic neoplasm (SCN). They each show distinct biological behaviour with different risk of progression and risk for malignant transformation. PCN are a challenging clinical entity, often incidentally encountered (2-45% of general population) with ever improving imaging modalities. In these patients, cancer prevention needs to be carefully balanced against overtreatment. The presented European guidelines deal with all common forms of PCN and give evidence-based suggestions for diagnosis and management.
Recommendations
Diagnosis
- Biomarkers
Due to their lack of ability to identify high-grade dysplasia or cancer, no serum biomarkers are currently available to further discriminate PCN. In cases of IPMN with concern for malignant transformation, CA 19-9 levels may be considered. Next-generation sequencing for analysis of KRAS and GNAS mutations in cyst fluid has shown promising results identifying mucin producing cysts and may be considered if the diagnosis is unclear.
- Radiology
MRI/MRCP with an accuracy between 40-95% represents the imaging modality of choice in PCN, as it has proven more sensitive than CT (accuracy 40-81%). Nevertheless, specificity and accuracy in identifying specific PCN type remains low for both modalities, especially in small lesions. MRI is the preferred imaging modality for follow-up of PCN. In certain cases, such as assessment of calcifications in chronic pancreatitis, suspicion of malignancy and for the assessment of vascular involvement, multimodal imaging including CT has proven beneficial.
- Endoscopy
In PCN showing features of concern (clinical or radiological), endoscopic ultrasound (EUS) is recommended as an adjunct to other imaging modalities. EUS helps with the identification of features raising concern for malignant transformation. Contrast enhanced-EUS is superior to standard EUS in identifying features indicating malignant potential, such as mural nodules, hyperenhancement, solid mass or septations. If radiologic imaging is unclear, EUS-guided fine-needle aspiration (FNA) may be added to improve diagnostic accuracy to distinguish between mucinous versus non-mucinous PCN and benign versus malignant PCN. EUS should only be performed when results are expected to change clinical management and not in the case of high risk for bleeding.
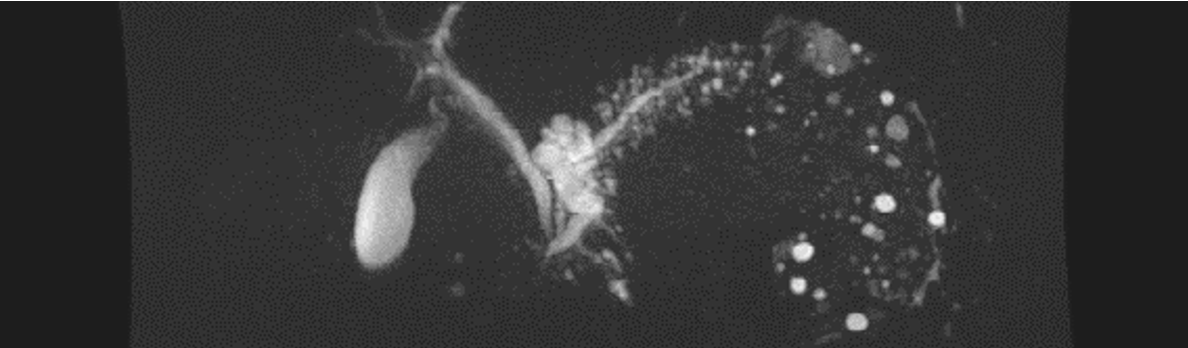
Figure 1a.: Polylobulated 4.5x2.3cm mixed-type IPMN in the pancreatic head with dilatation of the main pancreatic duct up to 11mm. Histology confirmed highgrade dysplasia
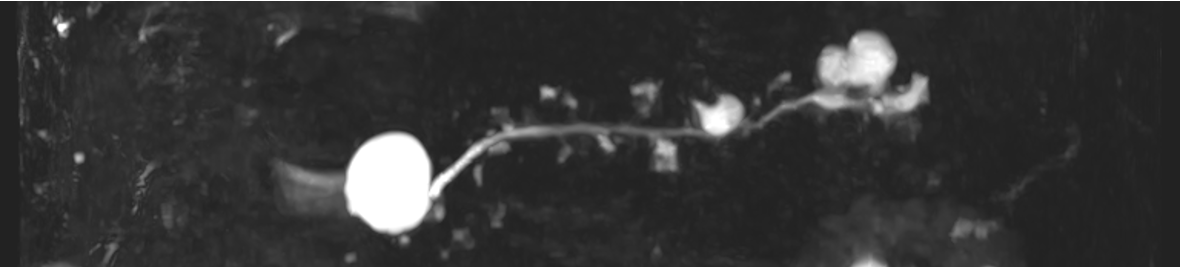
Figure 1b.: Patient with two branch-duct IPMN, 3.0cm in the pancreatic head and 2.5cm in the pancreatic tail, both cysts without other risk factors.
Management
- Intraductal papillary mucinous cystic neoplasms (IPMN)
Patients with main-duct (MD) IPMN have a high risk for malignancy and should be resected, if fit for surgery. Mixed-type IPMN have a similar high risk for malignancy as MD-IPMN and resection is again advised, if the patient is fit for surgery (Figure 1a). In branch-duct (BD) IPMN, the rate of malignant transformation is subject to different risk factors (Figure 1b). The following risk factors need to be carefully evaluated as even small IPMN may progress to high-grade dysplasia or cancer (Figure 2). Absolute criteria for resection of BD-IPMN are cyst related jaundice, positive cytology for high-grade dysplasia/cancer, main duct dilatation ≥10mm, mural nodules ≥5mm or presence of a solid mass. Relative criteria for resection of BD-IPMN are a cyst diameter ≥40mm, growth rate ≥5mm/year, clinical symptoms such as acute pancreatitis or new onset of diabetes mellitus, an increased CA 19-9, main duct dilatation ≥5mm or mural nodules <5mm. Patients with IPMN and no indication for surgical resection should be followed with MRI during the first year every 6-months and yearly afterwards. In patients with a relative surgical indication a 6-month follow-up is recommended. Importantly, a change in clinical symptoms should trigger prompt evaluation. Follow-up in IPMN patients should continue until they are no longer fit for surgery. In patients with an absolute indication for surgery an oncologic resection including standard lymphadenectomy should be performed. In patients with a BD-IPMN with relative indication for surgery, oncologic resection is again indicated for most cases. Frozen section of the pancreatic resection margin should routinely be performed and resection should continue up to total pancreatectomy, if high-grade dysplasia or cancer is found at the surgical margin. Low grade dysplasia at the surgical margin does not require further resection. After surgical resection lifelong surveillance is recommended as long as the patients is fit and willing to undergo surgery if indicated.
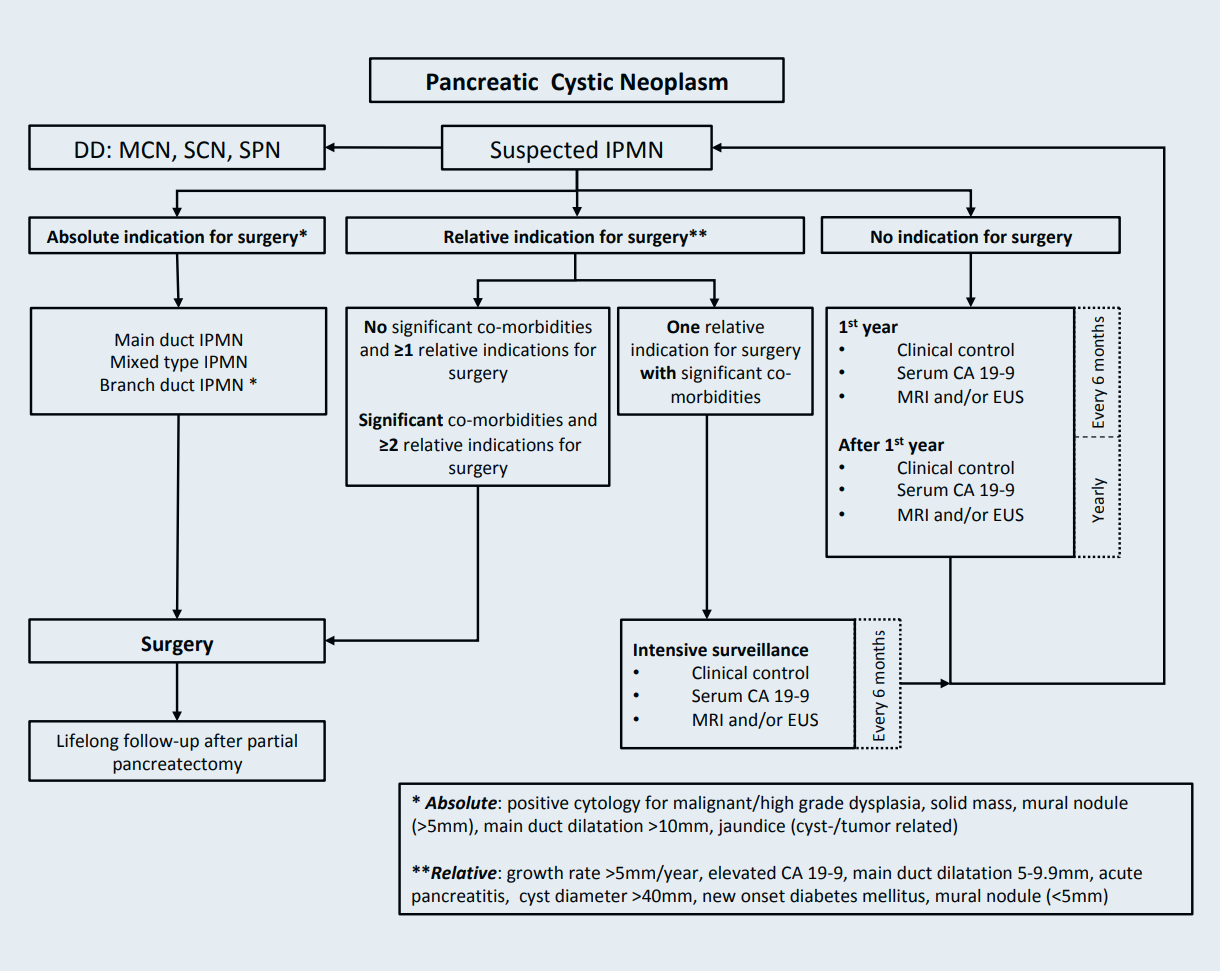
Figure 2: Management algorithm of IPMN. Modified from «European Study Group on Cystic Tumours of the Pancreas. Gut. 2018». (EUS, endoscopic ultrasound; IPMN, intraductal papillary mucinous cystic neoplasms; MCN, mucinous cystic neoplasm; MRI, magnetic resonance imaging; SCN, serous cystic neoplasm; SPN, solid papillary neoplasia.)
- Mucinous cystic neoplasm (MCN)
Patients with MCN may either undergo resection or lifelong surveillance, as long as they are fit for surgery. Resection is indicated when the cystic lesion is ≥ 40mm, the patient is symptomatic or when risk factors such as mural nodules are present. Surgery includes standard oncologic pancreatic resection with lymphadenectomy. In absence of the above-mentioned risk factors, follow-up imaging every 6 months for the first year, then annually remains an option. Of note, MCN growth rate should be taken into consideration in the decision-making process.
- Serous cystic neoplasm (SCN)
SCN represents a benign entity, specific mortality due to SCN is nearly zero. Asymptomatic patients with SCN should be followed-up for one year, afterwards a symptom-based follow-up is recommended. In spite of its slow growth rate and reported stable size in most patients, rarely symptoms arise due to compression of adjacent organs, making decompressive surgery a valuable treatment option in these cases.
Conclusion
Despite improved imaging modalities, differentiation of various types of PCN with their respective risk of malignant transformation remains a challenge. Patients with PCN should be discussed in multidisciplinary tumour boards in centers with appropriate expertise in both diagnosis and treatment. The European evidence based guidelines should provide a structured algorithm for diagnosis and treatment.






